NOTE: This article was originally posted on May 31, 2026, and was updated on July 27, 2026
Can Higher Blood Sugar in Type 2 Diabetes Be Due to Protein?
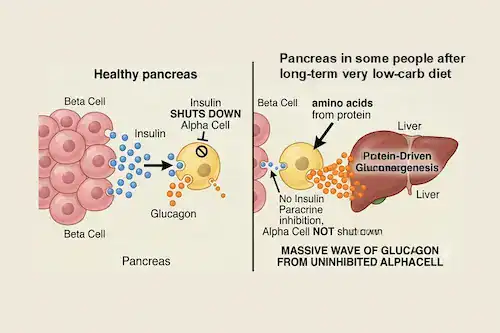
Prolonged carbohydrate restriction, such as a long-term keto diet, greatly reduces daily baseline insulin, causing pancreatic beta cells to scale down insulin release. This significant drop in insulin removes the vital local ‘paracrine brake’ that insulin normally would apply to the alpha cells of the pancreas, leaving them uninhibited and free to drive the liver to make glucose (gluconeogenesis).
Practitioner’s Preface
Carbohydrates have been the main macronutrient of interest in managing blood sugar in type 2 diabetes because of their direct impact on blood glucose levels; however, looking at long-term clinical data, there is a need to recognize the effect of dietary protein on pancreatic islet cells (both alpha and beta cells). This effect plays a key role in the secretion of the hormones insulin and glucagon, and in some people makes protein a significant regulator of blood glucose levels in people with type 2 diabetes.
Many individuals have successfully managed their blood sugar over the long-term by following a very-low-carbohydrate or a low-carbohydrate diet, but some of them have found that after several years, they are faced with a puzzling shift where the same low-carbohydrate, moderately-high-protein meals they have eaten for years now trigger unexpected blood glucose spikes. As outlined in this previous article titled Blood Sugar May Increase After Years on a Ketogenic Diet in Type 2 Diabetes, this occurs when dietary adherence to a very-low-carbohydrate (ketogenic) diet is flawless. That is, the rise in blood glucose is not due to “carb creep” but due to the liver-pancreatic alpha cell axis.
How Can a Long-Term Keto Diet Result in Higher Blood Sugar?
In healthy individuals, the pancreatic alpha cells and pancreatic beta cells exist in a tightly regulated paracrine relationship where one cell secretes chemical messengers that diffuse through the extracellular space to affect the nearby target cell.
In healthy individuals, when insulin rises, glucagon release is suppressed. When healthy people eat, their beta cells secrete insulin, which is communicated to the alpha cells of the pancreas and signals them to stop secreting the hormone glucagon. The insulin that is released locally within the pancreas acts as an immediate, powerful biological “brake” that shuts down glucagon secretion from the alpha cells.
In individuals diagnosed with type 2 diabetes, the pancreatic beta cells release insufficient amounts of insulin due to beta cell dysfunction. When dietary carbohydrate is restricted, blood sugar is initially reduced, but so is the daily demand for insulin. This drop in daily insulin production results in a low insulin-to-glucagon ratio.
The previous article outlined that the DiRECT trial (Diabetes Remission Clinical Trial) identified a subset of 10% to 15% of people with type 2 diabetes as “non-responders” who lacked a first-phase insulin response and had lower baseline fasting insulin. Together, these factors fail to adequately inhibit pancreatic alpha cells, resulting in dietary protein spiking blood glucose. Some individuals who have been successfully following a very low-carb diet over an extended period of time experience something similar.
The lack of a robust localized insulin surge from the pancreatic beta cells removes the “paracrine brake” on the pancreatic alpha cells, and over an extended period of time on a low-carbohydrate, moderately high-protein meal, there is insufficient insulin release from the pancreatic beta cells to inhibit glucagon release from the alpha cells, leaving the alpha cells uninhibited. When the amino acids from dietary protein enter the bloodstream, they stimulate these unmoderated alpha cells to hypersecrete glucagon, and when the liver is exposed to a wave of glucagon, it is signaled to ramp up gluconeogenesis, turning those amino acids directly into glucose.
How Does Type 2 Diabetes Change Response to Protein?
Type 2 diabetes alters the response to protein consumption due to blunted insulin release and a structurally reduced insulin-to-glucagon ratio. Clinical research reveals that a protein’s digestion rate significantly determines blood sugar response after a meal (postprandial glycemic outcome), with fast-digesting proteins resulting in uninhibited glucagon spikes.
A recent review published in January 2026 titled “Effects of protein intake on glucagon, insulin, and glucose dynamics: implications for diabetes” [1] provides the biochemical evidence to explain this phenomenon [2,3]. This review reported that the response to protein consumption is altered in diabetes [1].
A 1975 study of untreated individuals with type 2 diabetes who underwent an arginine infusion test displayed higher glucagon and lower insulin secretion compared to non-diabetic controls, which contributed to significantly higher blood glucose levels [4]. When the same individuals repeated the arginine infusion test after 8 weeks of diet, insulin, or sulfonylurea therapy, their glucagon and insulin responses were improved, but still remained worse than the control group without type 2 diabetes. In addition, the individuals with type 2 diabetes continued to display a reduced insulin-to-glucagon ratio compared to the control group without type 2 diabetes [4], which may account for differences in response to protein intake in those with type 2 diabetes.
The effect of dietary protein on alpha cells in those with type 2 diabetes is influenced by differences in amino acid composition related to whether the protein is from plant versus animal sources, as well as rates of digestion [5]. A 2015 systematic review and meta-analysis found that replacing 35% of total protein per day with plant protein for 8 weeks significantly lowered HbA1c levels as well as fasting insulin levels in people with type 2 diabetes [6]. In general, plant proteins are slower-digesting, while animal proteins are fast-digesting; rapidly digested proteins typically result in a greater glucose excursion and a more immediate insulin and glucagon response [7]. Exceptions include casein (a slow-digesting animal protein) and pea protein (faster digesting than other plant proteins).
While some meta-analyses [6] attributed the blood sugar benefits to eating more plant-based proteins, the difference may stem from increasing the ratio of slowly-digesting proteins to fast-digesting proteins that make up the diet. For example, following a six-week diet of either pea plant protein (medium-fast digesting) or casein animal protein (slow digesting protein), the casein group was associated with improved insulin sensitivity and secretion, as well as lower 4-hour insulin and glucagon [5]. The authors of the review believe that
“A protein’s rate of digestion is a stronger indicator of its glycemic response than its origin (plant versus animal)” [1].
In individuals with type 2 diabetes, where there is insulin resistance and where insulin secretion is often blunted, the differing response to protein sources, amount, and absorption rates needs to be considered. This is where clinicians such as myself can design highly targeted Meal Plans to help stabilize uninhibited alpha cells by lowering glucagon release and increasing appropriate insulin release.
Why Does Eating Protein Without Carbohydrate Trigger Blood Glucose Spikes?
Consuming protein in isolation alters the islet-hormone profile because amino acids preferentially stimulate glucagon hypersecretion over insulin release, resulting in an elevated glucagon-to-insulin ratio. However, combining protein with complex carbohydrates activates a synergistic insulin response that effectively offsets the amino-acid-stimulated glucagon wave.
The timing of protein intake can help control for blood sugar excursions. Eating protein in the absence of carbohydrate stimulates both glucagon and insulin secretion [8], and in healthy individuals without type 2 diabetes, amino acids tend to preferentially stimulate glucagon secretion over insulin secretion, resulting in a lower insulin-to-glucagon ratio and a higher blood glucose level; however, when protein consumption is combined with carbohydrate, it reduces the carbohydrate-induced rise in blood sugar.
Studies have found that blood glucose levels are typically lower following dietary intake of amino acids along with carbohydrates compared to eating carbohydrates alone [9], and this is attributed in part to carbohydrate’s ability to trigger a synergistic, robust spike in insulin production that offsets the amino acid-stimulated glucagon release [9].
Protein stimulates pancreatic alpha-cells to secrete glucagon more strongly than pancreatic beta-cells to secrete insulin, which means that a high intake of protein will result in a higher glucagon-to-insulin ratio. Long-term higher habitual protein intake may result in higher levels of blood glucose. Anecdotally, I have observed this rise in overall blood glucose in some individuals who were previously diagnosed with type 2 diabetes and who have been following a carnivore diet.
In a study comparing individuals without type 2 diabetes who maintained an average protein diet of 0.57-0.80g/kg/day versus those who maintained a high protein diet of 1.25-2.41g/kg/day for at least six months, the high protein group released significantly more insulin and glucagon [10], as well as a 12% higher glucose at low plasma insulin concentration [10].
Given the higher blood glucose levels associated with type 2 diabetes, the overall amount of protein being consumed must be factored in, as well as whether the protein is quickly digested or slowly digested.
What Can Help Restore the Pancreatic Paracrine Brake?
Restoring the local paracrine brake on hyperactive alpha cells requires nutritional interventions: maintaining a moderate protein threshold (0.80 g/kg/day), prioritizing slow-digesting whole-food matrices, intentionally pairing proteins with fat and fiber to delay amino acid absorption, and executing the 10-minute rule with a micro-dose of complex carbohydrates to trigger a corrective insulin pulse.
For individuals who were previously diagnosed with type 2 diabetes and who have been experiencing an ongoing rise in blood glucose after years on a very-low-carbohydrate (ketogenic) diet (30-50 g of carbohydrate/day), understanding the lack of insulin suppression by the pancreatic beta cells on the pancreatic alpha cells is key. The solution is not further carbohydrate restriction or adopting a carnivore diet, which would result in a much higher intake of dietary protein in the absence of dietary carbohydrate intake.
Clinical Application
In designing Meal Plans for people who have put their type 2 diabetes into remission on a very low carb/keto diet, I implement a few key dietary strategies to help them begin to restore the pancreatic paracrine brake as much as possible. This helps calm uninhibited gluconeogenesis from their alpha cells. Some of these strategies include:
- A moderate protein intake of 0.80 g/kg/day, if appropriate, and if a higher protein intake is required, such as in the case of older adults to prevent sarcopenia, distributing protein intake evenly throughout the day in meals not above 30g of protein per day and implementing the strategies below.
- Prioritizing real whole food sources of protein (over rapidly digested protein powders or amino acid isolates) and prioritizing slowly digesting protein sources (plant- or animal-based), while avoiding fast-digesting protein sources.
- Incorporating structural dietary “brakes” on the pancreatic alpha cells by avoiding eating protein foods in isolation, and also intentionally pairing protein foods with other nutritional components, including fat and fiber, which significantly slows the absorption rate of amino acids.
- Simulating the First-Phase Insulin response by ingesting a small amount of a slowly metabolized carbohydrate 10 minutes before a meal that has protein. This very small amount of carbohydrate triggers non-competitive inhibition of the alpha cells, which quiets glucagon hypersecretion and, over time, will prevent unregulated liver gluconeogenesis.
More Info
If you would like dietary support to better manage your blood sugar levels, you can learn about me and the Comprehensive Dietary Package that I offer.
To your good health.
Joy
You can follow me on:
Twitter: https://twitter.com/jyerdile
Facebook: https://www.facebook.com/BetterByDesignNutrition/
Support for Rising Blood Sugar in Type 2 Diabetes
If you have been experiencing rising blood sugar levels despite adherence to a very low-carbohydrate or low-carbohydrate diet, I can design a Meal Plan for you that implements the strategies discussed in this article.
Quick Clinical Summary
Q: How does protein intake cause blood sugar spikes in long-term low-carb or ketogenic diets?
A: Prolonged carbohydrate restriction drastically reduces daily baseline insulin release. In a biological subset of individuals with type 2 diabetes, this drop removes the vital local ‘paracrine brake’ that insulin applies to neighboring alpha cells. Without insulin suppression, incoming amino acids from dietary protein heavily stimulate the alpha cells to hypersecrete glucagon, driving the liver to aggressively run gluconeogenesis and convert those amino acids into glucose.
Q: Does the protein source alter the glycemic and glucagonocentric response in T2D?
A: Yes, but clinical research indicates that a protein’s rate of digestion is a stronger indicator of its glycemic response than its literal biological origin (plant vs. animal). Fast-digesting proteins cause a rapid, sharp glucose excursion and immediate glucagon response, whereas slow-digesting proteins (such as animal-derived casein or fiber-bound plant proteins) help regulate islet-hormone dynamics more safely.
Q: What is a nutritional component strategy to restore the paracrine brake on uninhibited alpha cells?
A: Key clinical strategies include keeping protein intake moderate (around 0.80 g/kg/day), intentionally pairing protein with fats and fibers to slow amino acid absorption, avoiding fast-digesting protein powders, and strategically ingesting a very small amount of slowly metabolized carbohydrate 10 minutes before a meal. This minor carb intake stimulates a localized, first-phase-like insulin release that effectively quiets glucagon hypersecretion.
Q: Why does eating protein in the complete absence of carbohydrates alter the insulin-to-glucagon ratio?
A: Dietary protein naturally stimulates pancreatic alpha cells to secrete glucagon much more robustly than it stimulates beta cells to release insulin. When protein is consumed entirely in isolation, it yields a high glucagon-to-insulin ratio that favors endogenous glucose production. However, when paired correctly with structured carbohydrates, the carbohydrate component actively suppresses the amino-acid-stimulated glucagon wave.
Found this article of interest? Be sure to read: Alpha Cell Dominance: What Is It and How to Address It
References
- Nagy S, Turner LV and Riddell MC. Effects of protein intake on glucagon, insulin, and glucose dynamics: implications for diabetes. Front. Clin. Diabetes Healthc. 2026 Jan 12;6:1712506. doi: 10.3389/fcdhc.2025.1712506.
- Yanagisawa Y. How dietary amino acids and high protein diets influence insulin secretion. Physiol Rep. (2023) 11:e15577. doi: 10.14814/phy2.15577.
- Paterson MA, Smart CEM, Lopez PE, Howley P, McElduff P, Attia J, et al. Increasing the protein quantity in a meal results in dose-dependent effects on postprandial glucose levels in individuals with Type 1 diabetes mellitus. Diabetic Medicine. (2017) 34:851–4. doi: 10.1111/dme.13347.
- Ohneda A, Ishii S, Horigome K, Yamagata S. Glucagon response to arginine after treatment of diabetes mellitus. Diabetes. (1975) 24:811–9. doi: 10.2337/diab.24.9.811.
- Markova M, Hornemann S, Sucher S, Wegner K, Pivovarova O, Rudovich N, et al. Rate of appearance of amino acids after a meal regulates insulin and glucagon secretion in patients with type 2 diabetes: A randomized clinical trial. Am J Clin Nutr. (2018) 108:279–91. doi: 10.1093/ajcn/nqy100.
- Viguiliouk E, Stewart SE, Jayalath VH, Ng AP, Mirrahimi A, De Souza RJ, et al. Effect of replacing animal protein with plant protein on glycemic control in diabetes: A systematic review and meta-analysis of randomized controlled trials. Nutrients. (2015) 7:12. doi: 10.3390/nu7125509.
- He T, Giuseppin MLF. Slow and fast dietary proteins differentially modulate postprandial metabolism. Int J Food Sci Nutr. (2014) 65:386–90. doi: 10.3109/09637486.2013.866639.
- Gerich JE, Charles MA, Grodsky GM. Characterization of the effects of arginine and glucose on glucagon and insulin release from the perfused rat pancreas. J Clin Invest. (1974) 54(4):833–41. doi: 10.1172/JCI107823.
- Nuttall FQ, Schweim KJ, Gannon MC. Effect of orally administered phenylalanine with and without glucose on insulin, glucagon and glucose concentrations. Hormone Metab Res. (2006) 38:518–23. doi: 10.1055/s-2006-949523.
- Linn T, Santosa B, Grönemeyer D, Aygen S, Scholz N, Busch M, et al. Effect of long-term dietary protein intake on glucose metabolism in humans. Diabetologia. (2000) 43:1257–65. doi: 10.1007/s001250051521.


I am a Registered Dietitian Nutritionist and the owner of BetterByDesign Nutrition Ltd. With a postgraduate degree in Human Nutrition and a background as a published mental health nutrition researcher, I have been dedicated to supporting my clients’ clinical needs since 2008.
I hold active professional licenses in BC (CHPBC), Alberta (CDA), and Ontario (CDO), allowing me to provide regulated Medical Nutrition Therapy across these provinces. My expertise spans chronic disease management, complex digestive health, and therapeutic diets. I am deeply passionate about helping people reclaim their health, rooted in my firm belief that Nutrition is BetterByDesign©.