Practitioner’s Preface
There are four documented ways to put type 2 diabetes into remission: a very low-calorie diet [1,2,3], bariatric surgery (especially the use of the Roux-en-Y procedure) [4,5], a ketogenic diet [6,7], and use of GLP-1 agonists such as semaglutide, dulaglutide, and tirzepatide [8]. Each comes with advantages and limitations.
There is strong one- and two-year clinical data demonstrating that a very-low-carbohydrate/ ketogenic diet is both safe and effective for achieving remission of type 2 diabetes symptoms; however, there is limited long-term data. As outlined in a previous article titled Blood Sugar May Increase After Years on a Ketogenic Diet in Type 2 Diabetes, the five-year Virta Health data showed that the average HbA1c for those completing the study averaged ~7.3%, which was up from 6.3% at a year, and 6.7% at two years [9]. An 8-year dataset from UK-based General Practitioner Dr. David Unwin’s practice found that HbA1c tended to drift or worsen as time went on [10].
While “carb creep” (increased carbohydrate consumption) may explain the blood sugar rise for many people, these data do not account for individuals who continue to follow ketogenic carbohydrate restriction yet whose blood glucose begins to rise anyway. The rise in blood glucose results from the liver-pancreatic alpha cell axis, which is explained by Dr. Roger Unger’s bi-hormonal theory of diabetes [11,12,13]. Understanding this mechanism allows for some simple long-term strategies to help those who were previously in remission of type 2 diabetes symptoms to better control their blood sugar levels.
How Do Pancreatic Alpha and Beta Cells Control Blood Sugar After Meals?
In healthy metabolic function, pancreatic alpha and beta cells maintain a tightly regulated paracrine relationship that controls blood glucose levels. When food is consumed, beta cells secrete a rapid localized burst of insulin that acts as an immediate biological brake to suppress glucagon secretion from neighboring alpha cells, preventing unwanted liver glucose production.
To understand this local cellular communication, picture one cell secreting chemical messengers that diffuse through the extracellular space to affect the nearby target cell. In healthy individuals, when insulin rises, glucagon release is suppressed. When healthy people eat, their beta cells signal the alpha cells of the pancreas to stop secreting the hormone glucagon.
When someone hasn’t eaten for a while, blood sugar falls, alpha cells release glucagon that binds to receptors on liver cells, and this triggers a rapid enzyme cascade (via cyclic AMP) that converts stored glycogen into glucose (glycogenolysis), releasing it into the bloodstream to fuel the brain, muscles, and organs.
If fasting is prolonged and glycogen stores run low, glucagon released from the alpha cells signals the liver to manufacture glucose from scratch using circulating amino acids from protein (gluconeogenesis), and makes glucose from the glycerol backbone of triglycerides derived from fat, via the glycerol pathway.
Why Does Blood Sugar Tend to Get Higher After a Long-Term Ketogenic Diet?
Extended adherence to a very-low-carbohydrate ketogenic diet drastically minimizes systemic insulin demand, causing pancreatic beta cells to scale down baseline insulin production progressively. This relative insulin deficiency removes the vital paracrine brake on neighboring alpha cells, letting glucagon release go completely unchecked and signaling the liver to accelerate both glycogenolysis and gluconeogenesis from fats and protein.
This baseline relative insulin deficiency (compared to glucagon) explains why people who were diagnosed several years ago with type 2 diabetes and who have followed a very-low-carbohydrate (keto diet) for an extended period begin to experience a glucose spike after eating a meal that is low in carbohydrate, but high in protein. The sudden influx of amino acids stimulates the uninhibited alpha cells to release glucagon. Since insulin release is too low due to long-term carbohydrate restriction, there is no countersignal to stop the liver from breaking down glycogen and overproducing glucose.
How Does Eating Protein Affect the Insulin-to-Glucagon Ratio?
Consuming dietary protein in the absolute absence of carbohydrates inherently biases pancreatic secretion in favor of glucagon over insulin, driving down the insulin-to-glucagon ratio. Because amino acids trigger alpha cell activity much more intensely than beta cell activity, eating “naked” or fast-digesting protein sources forces the body into a high-glucagon state that prompts significant post-meal blood glucose excursions.
Even in healthy individuals without type 2 diabetes, eating protein foods in the absence of carbohydrates stimulates both insulin and glucagon, but amino acids inherently favor glucagon secretion over insulin [15]. This shift creates a lower insulin-to-glucagon ratio, resulting in higher blood glucose. Over the long term, maintaining a moderate to high-protein intake without sufficient dietary carbohydrates shifts the body permanently into this higher glucagon-to-insulin state.
Why Are Some Individuals with Type 2 Diabetes Non-Responders to Long-Term Keto?
Roughly 10% to 15% of individuals with type 2 diabetes exhibit a biological phenotype where advanced beta-cell dysfunction prevents the recovery of a rapid, first-phase insulin spike. When these individuals restrict carbohydrates long-term, their baseline insulin drops exceptionally low, leaving over-reactive pancreatic alpha cells entirely free to hypersecrete glucagon and drive aggressive liver gluconeogenesis whenever dietary protein is introduced.
For individuals previously diagnosed with type 2 diabetes, the pancreatic beta cells release insufficient amounts of insulin due to beta cell dysfunction. As outlined in a previous article, in these non-responders, the beta cells have crossed a “point of no return” and can not secrete a rapid burst of local insulin anymore, pointing to more exhausted baseline beta-cell function before intervention.
- The lack of a robust localized insulin surge from the pancreatic beta cells removes the “paracrine brake” on the pancreatic alpha cells. Over an extended period of time on a very low-carbohydrate, moderately high-protein diet, there is insufficient insulin release to inhibit glucagon release from the alpha cells, leaving the axis entirely uninhibited.
- When the amino acids from dietary protein enter the bloodstream, they stimulate these unmoderated alpha cells to hypersecrete glucagon, and when the liver is exposed to a wave of glucagon, it is strongly signaled to ramp up gluconeogenesis, turning those amino acids directly into glucose.
- The solution is not to restrict carbohydrates further, or to adopt a carnivore diet. Eliminating carbohydrates floods the body with more amino acids from protein, amplifying the uninhibited glucagon release and worsening the problem.
- The key is to restore the pancreatic paracrine “brake” and calm down the unregulated glucose production coming from the alpha cells.
How high can blood sugar rise from eating only protein and low-carb veggies?
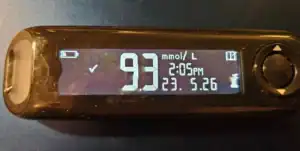
Everyone’s blood glucose response to foods is different, but having eaten low-carb for years and having previously put type 2 diabetes into remission (March 2019-March 2021) and continuing to eat low-carb, this is the blood glucose response I had on May 26, 2026, after eating 6 oz. of coho salmon with asparagus and mushrooms, without eating any carbs. My blood sugar before the meal was 5.2 mmol/L (94 mg/dl) and rose to 9.3 mmol/L (167 mg/dL) after 2 hours. My mistake was thinking that coho salmon was a ‘fatty fish’ (see below for explanation).

I recently made the same meal, except this time I ate 1 tbsp. cold, cooked barley 10 minutes beforehand, and my blood sugar was 5.7 mmol/L (103 mg/dl) 2 hours afterwards. The explanation as to why this worked is below.

What Are Some Practical Dietary Strategies That Help Stabilize Blood Glucose?
Restoring metabolic balance and halting glycemic drift requires dietary strategies that intentionally stimulate a micro-dose of pre-meal insulin to re-engage the pancreatic paracrine brake. This is achieved by utilizing the “10-Minute Rule” to mimic a first-phase insulin pulse with a precise quantity of complex, slowly metabolized carbohydrates, prioritizing slow-digesting whole-food protein matrices, and gradually adjusting the daily carbohydrate threshold.
To counteract the relative insulin deficiency of type 2 diabetes and long-term carbohydrate restriction, below are the practical frameworks that can help.
1. Simulate the “First-Phase Insulin Response”
Healthy individuals have what is called “the first-phase insulin response,” which is a rapid, intense burst of pre-stored insulin within the first 5 to 10 minutes of glucose entering the bloodstream. This pre-stored insulin released from the beta cells acts as a metabolic brake on the alpha cells, suppressing glucose production in the liver, preventing a sharp spike in blood sugar.
Individuals diagnosed with type 2 diabetes lack a first-phase response because their pancreatic beta cells release insufficient amounts of insulin due to beta cell dysfunction. Even when dietary carbohydrate is restricted over a long period of time, this first-phase insulin response is not restored, and daily demand for insulin is further suppressed. Simulating this first-phase response before a protein-containing meal is eaten helps restore that vital brake, and the timing of this targeted carbohydrate intake is critical.
The 10-Minute Rule
Eating a small amount of slowly metabolized carbohydrates 10 minutes before eating a meal that contains protein coaxes the pancreatic beta cells to release a small pulse of insulin before the meal. This inhibits the pancreatic alpha cells, quieting glucagon hypersecretion. Forcing the beta cells to release insulin before eating a protein-containing meal prevents the liver from overproducing glucose and reduces post-meal blood sugar spikes, reducing unregulated liver gluconeogenesis over time.
I have found that 2-3 blackberries, or a tablespoon of cold, cooked barley (a resistant starch), provide just enough complex structure, fiber, or resistant starch to gently nudge the beta cells to release a small amount of insulin without causing an independent blood sugar spike. Other examples are one tablespoon of cold cooked lentils or chickpeas, or 3 to 4 pods of cooked edamame (soybeans). The key to these examples lies in their physical matrix (fiber and resistant starch) and a micro-dose quantity.
2. Optimize Macronutrients
For individuals who were previously diagnosed with type 2 diabetes and who have been experiencing a rise in blood glucose after years on a very-low-carbohydrate (ketogenic) diet (30-50 g of carbohydrate/day), changing the types of proteins and amount of carbohydrate can help control blood sugar spikes.
- Moderate Protein Intake: Keep protein to a moderate intake of 0.80 g/kg/day, and if a higher protein intake is required, such as in the case of older adults to prevent sarcopenia, distribute protein intake evenly throughout the day in meals not above 30g of protein per day, while limiting protein sources that are high in the amino acids arginine, alanine, glycine which trigger gluconeogenesis the most of any amino acids [14-20].
- Prioritize Real, Whole Foods: Prioritize eating real, whole-food sources of protein over rapidly digested protein powders or amino acid isolates.
- Avoid Quickly Digested Protein: Avoid protein foods that are quickly digested, such as egg whites, lean white fish like cod, tilapia, haddock, and skinless chicken breast. Reach for protein foods that naturally come with fat, including whole eggs, fatty fish like king salmon, mackerel, and sardines, and cuts of meat that include fat.
- Don’t Eat Protein “Naked”: Most people diagnosed with type 2 diabetes have been taught not to eat carbs “naked”, but when alpha cells are over-reactive, it is important not to eat protein naked, either. Intentionally pair protein foods with healthy fats and fiber, which significantly slows down the absorption rate of amino acids into the bloodstream.
- Increase Overall Carbohydrates: Gradually transition from 30–50 grams of carbohydrate per day to a low-carbohydrate threshold between 80 and 100 grams of slowly digested carbohydrates per day.
Clinical Application
There is ample clinical data to support using significant dietary carbohydrate restriction for the first year or two to put the symptoms of type 2 diabetes into remission; however, maintaining long-term glucose control often requires a change in the types of proteins and the amount of carbohydrate eaten to counteract the effect of alpha cells driving unrestrained glucose production due to the suppressed and delayed insulin release.
More Info
If you would like dietary support to better manage your blood sugar levels after following a low-carb or very low-carb (keto) diet, please reach out. You can learn about me and the Comprehensive Dietary Package that I offer, along with specialized nutrition education teaching to help you know what to eat and when.
To your good health.
Joy
You can follow me on:
Twitter: https://twitter.com/jyerdile
Facebook: https://www.facebook.com/BetterByDesignNutrition/
Support for Rising Blood Sugar After Keto?
If you have been experiencing rising blood sugar levels despite adherence to a keto diet, I can design a Meal Plan for you that implements the strategies discussed in this article.
Quick Clinical Summary
Q: What is a first-phase insulin response and why is it a problem in people with type 2 diabetes?
A: A first-phase insulin response is the rapid, intense burst of pre-stored insulin that occurs in healthy people when they start to eat. Pre-stored insulin is released from the beta cells of the pancreas and acts as a metabolic “brake” on the pancreatic alpha cells and suppresses glucose production in the liver. People with type 2 diabetes lack a first-phase response because their pancreatic beta cells are dysfunctional.
Q: Why does a keto diet work for the first few years to control blood sugar in type 2 diabetes, but then blood sugar starts to rise again?
A: A keto (very-low-carbohydrate) diet works very well for the first few years to reduce blood glucose by significantly reducing dietary intake of carbohydrate. The problem is, type 2 diabetes is not only due to dysfunctional beta cells of the pancreas, but also alpha cells. In a long-term keto diet, eventually there is insufficient insulin released from the beta cells to suppress the oversecretion of glucagon from the alpha cells, which drives increasing blood glucose.
Q: What are some dietary strategies that can help calm overactive alpha cells in type 2 diabetes?
A: Two key dietary strategies to counteract overactive alpha cells include mimicking a first-phase insulin response by eating a small amount of slowly metabolized carbohydrates 10 minutes before eating a meal that contains protein, and changing the types of proteins that are eaten, and slightly increasing the amount of carbohydrate.
Found this article of interest? Be sure to read: Alpha Cell Dominance: What Is It and How to Address It
References
- Lim EL, Hollingsworth KG, Aribisala BS, Chen MJ, Mathers JC, Taylor R. Reversal of type 2 diabetes: normalisation of beta cell function in association with decreased pancreas and liver triacylglycerol. Diabetologia 2011;54:2506-14. doi:10.1007/s00125-011-2204-7 pmid:21656330
- Steven S, Hollingsworth KG, Al-Mrabeh A, et al. Very low-calorie diet and 6 months of weight stability in type 2 diabetes: pathophysiological changes in responders and nonresponders. Diabetes Care 2016;39:808-15. doi:10.2337/dc15-1942 pmid:27002059
- Lean ME, Leslie WS, Barnes AC, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. Lancet 2018;391:541-51
- Cummings DE, Rubino F (2018) Metabolic surgery for the treatment of type 2 diabetes in obese individuals. Diabetologia 61(2):257—264.
- Madsen, L.R., Baggesen, L.M., Richelsen, B. et al. Effect of Roux-en-Y gastric bypass surgery on diabetes remission and complications in individuals with type 2 diabetes: a Danish population-based matched cohort study, Diabetologia (2019) 62: 611. https://doi.org/10.1007/s00125-019-4816-2
- Hallberg SJ, McKenzie AL, Williams PT, Bhanpuri NH, Peters AL, Campbell WW, Hazbun TL, Volk BM, McCarter JP, Phinney SD, Volek JS. Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study.
- Athinarayanan, S. J., Adams, R. N., Hallberg, S. J., McKenzie, A. L., Bhanpuri, N. H., Campbell, W. W., Volek, J. S., Phinney, S. D., & McCarter, J. P. (2019). Long-term effects of a novel continuous remote care intervention including nutritional ketosis for the management of type 2 diabetes: A 2-year non-randomized clinical trial. Frontiers in Endocrinology, 10, 348. https://doi.org/10.3389/fendo.2019.00348
- Fadini GP, Giaccari A, Broglio F, Nollino L, Fattor B, Anichini R, Meregalli G, Avogaro A, Consoli A; GLIMPLES Study Investigators. Type 2 diabetes remission after initiation of GLP-1 receptor agonists: frequency, characteristics, and outcomes using multiple definitions in an observational study. Lancet Reg Health Eur. 2025 Oct 15;59:101499. doi: 10.1016/j.lanepe.2025.101499. PMID: 41142657; PMCID: PMC12550164.
- McKenzie AL, Athinarayanan SJ, Van Tieghem MR, Volk BM, Roberts CGP, Adams RN, Volek JS, Phinney SD, Hallberg SJ. 5-Year effects of a novel continuous remote care model with carbohydrate-restricted nutrition therapy including nutritional ketosis in type 2 diabetes: An extension study. Diabetes Res Clin Pract. 2024 Nov;217:111898. doi: 10.1016/j.diabres.2024.111898. Epub 2024 Oct 20. PMID: 39433217.
- Unwin D, Delon C, Unwin J, Tobin S, Taylor R. What predicts drug-free type 2 diabetes remission? Insights from an 8-year general practice service evaluation of a lower carbohydrate diet with weight loss. BMJ Nutrition, Prevention & Health. 2023;6:. https://doi.org/10.1136/bmjnph-2022-000544
- Unger RH, Aguilar-Parada E, Müller WA, Eisentraut AM. Studies of pancreatic alpha cell function in normal and diabetic subjects. J Clin Invest. 1970 Apr;49(4):837-48. doi: 10.1172/JCI106297. PMID: 4986215; PMCID: PMC322540. https://doi.org/10.1172/JCI106304
- Unger RH, Orci L. The essential role of glucagon in the pathogenesis of diabetes mellitus. Lancet. 1975 Jan 4;1(7897):14-6. doi: 10.1016/s0140-6736(75)92375-2. PMID: 46337.
- Unger RH, Cherrington AD. Glucagonocentric restructuring of diabetes: a pathophysiologic and therapeutic makeover. J Clin Invest. 2012 Jan;122(1):4-12. doi: 10.1172/JCI60016. Epub 2012 Jan 3. PMID: 22214853; PMCID: PMC3248306.
- Gerich JE, Charles MA, Grodsky GM. Characterization of the effects of arginine and glucose on glucagon and insulin release from the perfused rat pancreas. J Clin Invest. (1974) 54(4):833–41. doi: 10.1172/JCI107823.
- Linn T, Santosa B, Grönemeyer D, Aygen S, Scholz N, Busch M, et al. Effect of long-term dietary protein intake on glucose metabolism in humans. Diabetologia. (2000) 43:1257–65. doi: 10.1007/s001250051521.
- Boden, G., Rezvani, I., & Owen, O. E. (1984). Effects of glucagon on plasma amino acids. Journal of Clinical Investigation, 73(3), 785-793.
- Dean, E. D. (2019). A Primary Role for α-Cells as Amino Acid Sensors. Diabetes, 69(4), 542–549.
- Finan B, Capozzi ME, Campbell JE. Repositioning Glucagon Action in the Physiology and Pharmacology of Diabetes. Diabetes. 2020 Apr;69(4):532-541. doi: 10.2337/dbi19-0004. Epub 2019 Jun 9. PMID: 31178432; PMCID: PMC7085250.
- Galsgaard, K. D., Jepsen, S. L., Kjeldsen, S. A. S., et al. (2020). Alanine, arginine, cysteine, and proline, but not glutamine, are substrates for, and acute mediators of, the liver-α-cell axis in female mice. American Journal of Physiology-Endocrinology and Metabolism
- Nagy S, Turner LV and Riddell MC. Effects of protein intake on glucagon, insulin, and glucose dynamics: implications for diabetes. Front. Clin. Diabetes Healthc. 2026 Jan 12;6:1712506. doi: 10.3389/fcdhc.2025.1712506.


I am a Registered Dietitian Nutritionist and the owner of BetterByDesign Nutrition Ltd. With a postgraduate degree in Human Nutrition and a background as a published mental health nutrition researcher, I have been dedicated to supporting my clients’ clinical needs since 2008.
I hold active professional licenses in BC (CHPBC), Alberta (CDA), and Ontario (CDO), allowing me to provide regulated Medical Nutrition Therapy across these provinces. My expertise spans chronic disease management, complex digestive health, and therapeutic diets. I am deeply passionate about helping people reclaim their health, rooted in my firm belief that Nutrition is BetterByDesign©.