Introduction
As a Dietitian who supports people with food addiction, I was recently asked to speak at a food addiction summit. The evening before speaking, I was given a list of the questions I would be asked. The first one was “How has food addiction impacted your life? How old were you”? The opening question at the summit was “Do you identify as a food addict”?
Personal Experience with Trigger Foods
I had to really think about how to answer this. I knew there were two specific foods over which I had no “off button”. If you’ve listened to some of the podcasts I’ve spoken at, you will know that those two foods are hot Montreal-style bagels that are baked in a wood-burning oven, and pizza — but only ones baked in a wood-burning oven (or at a very high heat in a pizza oven). I have NO idea why these are like “kryptonite” to me, and can think of no memory that offers a clue. When I was a kid, there were “Cheezies ®” (a brand of cheese puff snack food from Canada — essentially they are extruded cornmeal covered in powdered cheddar cheese), and as a teenager, there was Nutella®. I would eat Cheezies or Nutella over a period of a few hours, until the container was empty.
Defining Food Addiction via DSM-5 Criteria
To answer the question, ‘how has food addiction impacted my life’, I first had to define ‘food addiction’. Since my post-graduate research was in the area of mental health nutrition, I turned to the Diagnostic and Statistical Manual (DSM-5), which is used to classify mental health disorders for diagnoses, treatment, and research. The DSM-5 recognizes substance use disorders [1] resulting from the use of 10 separate classes of drugs:
- alcohol;
- caffeine;
- cannabis;
- hallucinogens (such as LSD);
- inhalants;
- opioids;
- sedatives, hypnotics or anxiolytics (anti-anxiety medication);
- stimulants (including amphetamine-type substances, cocaine, etc.);
- tobacco;
- and other or unknown substances
Is food addiction a substance use disorder? I guess it depends on who one asks.
On one hand, one’s “kryptonite” foods could fall under “and other or unknown substances,” but as I mentioned in the summit, I don’t think it is the foods themselves that people become addicted to.
Neurobiology of Hyper-Palatable Foods
I believe that it is the release of dopamine from the pleasure center of the brain that is associated with the consumption of these foods, supported by endo-cannabinoids and endo-opioids that are also released.

Joy Erdile speaking at the Food Addiction Summit
The first question I was asked at the summit was whether I identified as a food addict. I referred to the list from the DSM-5, which lists the 11 criteria related to substance use disorder.
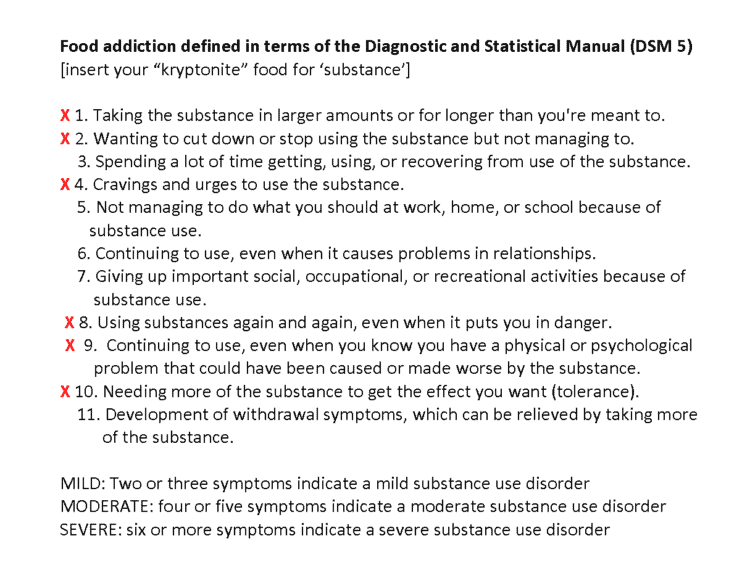
Food addiction in terms of the definition of substance use disorder (DSM-5)
Clinical Self-Assessment
In preparation for the talk, I had marked a red “x” beside the ones that applied to foods that I consider my “kryptonite”.
- Taking the substance in larger amounts or for longer than you’re meant to.
- Wanting to cut down or stop using the substance but not managing to.
- Spending a lot of time getting, using, or recovering from use of the substance.
- Cravings and urges to use the substance.
- Not managing to do what you should at work, home, or school because of substance use.
- Continuing to use, even when it causes problems in relationships.
- Giving up important social, occupational, or recreational activities because of substance use.
- Using substances again and again, even when it puts you in danger.
- Continuing to use, even when you know you have a physical or psychological problem that could have been caused or made worse by the substance.
- Needing more of the substance to get the effect you want (tolerance).
- Development of withdrawal symptoms, which can be relieved by taking more of the substance.
I could certainly remember eating more hot bagels or pizza than I wanted to, and for longer than I intended, so “yes” to criterion #1.
I certainly wanted to cut down or stop eating hot bagels or pizza, but did not manage to, so “yes” to criterion #2.
Criteria #3 was a “no”. I never spent a lot of time getting, using, or recovering from eating those (or any) foods.
There was no question, criterion #4 was a “yes”. I certainly had cravings and urges to eat these foods that only abated when I went low-carb and stopped eating them.
Criteria #5, #6, #7, and #11 were all “no”. Eating these (or any foods) did not interfere with me doing what I needed to at work, home, or school; they didn’t cause problems in relationships, and I didn’t give up any important social, occupational, or recreational activities because of them. I didn’t experience withdrawal symptoms when I ate those foods.
Physical Consequences and Remission

The reality of answering criteria #8 and #9 was undeniable. I ate foods such as bagels and pizza (and foods high in both carbs and fat) again and again — even when it put me in danger. I continued to eat these foods, even though I knew (but was in denial!) that I had several physical problems that could have been caused by or made worse by eating these foods.

I was obese, had type 2 diabetes and dangerously high blood pressure — and was a Registered Dietitian with a master’s degree who was in denial as to just how much danger I had put myself in!
Reading Dr. Vera Tarman’s book, Food Junkies, made me come face-to-face with criterion #10. I had given up milk chocolate when I adopted a low-carb lifestyle, but reading the book made me realize that I needed more dark chocolate to enjoy it. This was classic tolerance.
I met the criteria for ‘substance use disorder’ when I applied the definition of “substance’ to specific foods. In colloquial terms, I am a food addict. I don’t say “I am a type 2 diabetic” because I am in remission. I don’t say “I have hypertension or obesity” because I am in remission. So, more accurately, I am a person with food addiction, in remission.
Severity and Abstinence Strategies
Food addiction in terms of substance use disorder
If food addiction were classified as a ‘substance use disorder’, then meeting 6 of 11 criteria indicates it would be “severe”. But it’s only hot bagels and pizza! Does that make me a “food addict”? Here is a rhetorical question that may help answer this: Does it matter if an alcoholic is powerless over only one type of rum and one type of whiskey? I don’t think so.
Defining Abstinence in Food Addiction
One of the other questions I was asked during the summit was to define “abstinence” and what an “abstinence food plan” is. This is how I defined them;
“For me, abstinence is “the practice of restraining oneself from indulging in something”. There is alcohol-addiction, drug-addiction, gambling-addiction, sex-addiction, and food-addiction — but it is not possible to completely abstain from food, as it is necessary for survival. I define abstinence as “restraining from indulging in foods over which one has no control”.
Alcoholics Anonymous uses the term “powerless” to describe addiction, so I define abstinence as “restraining from foods over which one is powerless to stop eating.”
An “abstinent food plan” does not include foods over which a person is powerless to control the amount they eat.”
Final Thoughts…
The DSM-5 does NOT define “food addiction”. It defines “substance use disorder“. That said, I think that looking at whether specific foods or categories of food result in these types of symptoms can be helpful to consider. It can help one decide whether getting support for food addiction may provide a context and structure that they find helpful.
More Info
I design Meal Plans for people with food addiction and also support the dietary side of things for those working with a food addiction or sugar addiction counsellor, or in a 12-step program for food addiction.
Learn about me and the support that I can provide you with through the Comprehensive Dietary Package.
To your good health!
Joy
You can follow me on:
Twitter: https://twitter.com/jyerdile
Facebook: https://www.facebook.com/BetterByDesignNutrition/
References
- Hasin DS, O’Brien CP, Auriacombe M, et al. DSM-5 criteria for substance use disorders: recommendations and rationale. Am J Psychiatry. 2013;170(8):834-851. doi:10.1176/appi.ajp.2013.12060782 [https://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.2013.12060782]

© 2025 BetterByDesign Nutrition Ltd.

Joy is a Registered Dietitian Nutritionist and owner of BetterByDesign Nutrition Ltd. She has a postgraduate degree in Human Nutrition, is a published mental health nutrition researcher, and has been supporting clients’ needs since 2008. Joy is licensed in BC, Alberta, and Ontario, and her areas of expertise range from routine health, chronic disease management, and digestive health to therapeutic diets. Joy is passionate about helping people feel better and believes that Nutrition is BetterByDesign©.